I’ve been recuperating at home the last week or so, healing up after my fourth and FINAL breast reconstruction surgery (just need to “dot the i’s” and I’m done, folks – high five!). Anyway, like any good invalid, I’ve spent most of my time watching Netflix, devouring books and reading social media posts from friends, colleagues and fellow cancer buddies.
I especially liked But Doctor I Hate Pink’s recent call-to-arms, Pinktober, Metastasized, a series of blog posts that takes on a few of the more inane “awareness” campaigns that have popped up so far.
As most women with breast cancer can tell you, the month of October is a huge pink clusterfuck. There are your Boob-A-Thons, your giant bouncing boob races, your Save The Ta-Ta’s wet T-shirt contests (because women who’ve been forced to have mastectomies love nothing more than having healthy normal breasts shoved in their faces). Stores sell everything from pink clogs to pink stun guns with a fraction of the profits going towards yet more “awareness” as opposed to research which could, hello, save women’s LIVES not just their boobs. Even the NFL, which has so clearly demonstrated its love of women in recent days, gets into the act with pink cleats and pom-poms. As I mentioned, a clusterfuck.

Follow the bouncing boob. More importantly, follow the money.
Particularly annoying are the wrong-headed campaigns encouraging women, including survivors and metavivors (women with metastasized breast cancer who are not exactly “surviving” this crap) to post cryptic and vaguely sexual status updates on Facebook (“I like it on the floor!”), don T-shirts adorned with vapid boob-related slogans or bedazzle their bras (provided they still have them) with lace and sequins, again all in the name of breast cancer awareness.
But Doctor I Hate Pink does a great job of taking on these egregious offenders in her posts (she’s also started a cool new #mycancerisnot4sale social media campaign to fight the pink profiteering). “After five years of being truly, horribly sick, I can tell you that [breast cancer] is not a cute, fun little disease that you can play with or have a party about,” she writes. “Breast Cancer is the most trivialized disease in history … Do they have a tighty whitey decorating party for anal cancer? Let’s put a little brown glitter around the back end of the underwear, hey? Maybe some red sequins to show one of the signs that cancer lurks in that area? Yeah, let’s tell that cancer story through decoration.”
I love her feistiness and her humor and I especially love her point. You really don’t see other cancers – lung, liver, colon, bladder, prostate, anal, cervical, ovarian, etc. – being trivialized and/or sexualized in the same way that breast cancer has been over the last decade or so (although there is a rather interesting “put your cock in a sock” testicular cancer campaign currently rampaging through the interwebs).
What would it be like if other cancers were treated in the same ridiculous and demeaning fashion that some of these PR geniuses and clueless clods treat breast cancer? Read on to find out (with sincere apologies for those going through colon and testicular cancer). My edits are in italics. The rest is verbatim. As always, looking forward to your thoughts.
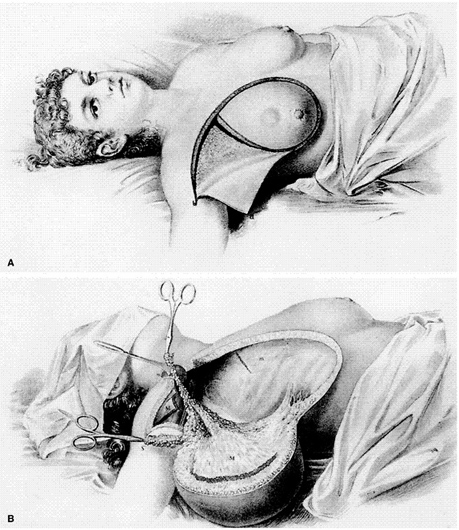
NATIONAL BRA (Breast Reconstruction Awareness) DAY promotion letter
Testicles are so much more than just “the boys” or “gonads.” They’re fabulous. They make us feel sexy, whether we’re in our best outfit, lounging around in our favorite flannel PJs, or just bare butt naked (sic). This fall, we want to spread this sensation of beauty and testicle empowerment to testicular cancer patients and survivors, as well as men nationwide.
Many men who undergo orchidectomy aren’t adequately informed about reconstruction options and reimbursement. In order to help raise awareness of these available options, we’re celebrating National TRA Day 2014 with a grassroots social media campaign using the hashtag #WHATSUNDERHERE.
Each participant receives a pair of boxer shorts with the #WHATSUNDERHERE hashtag on the front. In addition to the shorts, each kit comes with a set of cards with fun and thought-provoking sayings, such as: “Is Cancer Free,” “Looks Great Naked,” “Will Not Take Cancer Lying Down,” among others.
NATIONAL ‘NO BRA’ DAY – Facebook post from July 2011
Colons are Fantastic… We all think so. And what better way to express the way we feel than to support a full day of colon freedom?? Humans are magnificent creatures, and so are their colons. Let us spend the day unleashing colons from their colon zoos.
Support breast cancer? Really? Does this hideous disease really need our SUPPORT?
People, free your colons for 24 hours by removing those dreadful (but at times oh-so-helpful) underpants. Our poop chutes should not be hidden! It is time that the world see what we were blessed with. Your colons might be colossal, adorable, miniature, full, jiggly, fancy, sensitive, glistening, bouncy, smooth, tender, still blossoming, rosy, plump, fun, silky, Jello-like, fierce, jolly, nice, naughty, cuddly… But the most used adjectives to describe your colons on this day should be joyous, wild, and spectacular.
Everyone can participate! If you don’t want to free your colon, then your job will be to support everyone else by rocking something brown. It can be a brown tie, brown boxers, brown socks, a brown Colon Cancer Awareness Ribbon, I ♥ Colons Bracelet…. If it is brown, it supports us. (Your support means quite a lot to us…)
**If wearing underpants on this day is absolutely necessary, you can definitely show your support by wearing something brown.**
Yay for colons!

 So now there’s a pandemic. And my workplace and our scientists are right in the thick of it. I interviewed a couple of friends and Fred Hutch experts: one in infectious disease (Dr. Steve Pergam) and one in public health, health policy, outcomes AND oncology (Dr. Gary Lyman) to find out who’s most at risk for contracting COVID19.
So now there’s a pandemic. And my workplace and our scientists are right in the thick of it. I interviewed a couple of friends and Fred Hutch experts: one in infectious disease (Dr. Steve Pergam) and one in public health, health policy, outcomes AND oncology (Dr. Gary Lyman) to find out who’s most at risk for contracting COVID19.
 Discovered a new Twitter tool that I’m geeking out about a little. It’s called ‘Moments’ and it lets you string a bunch of tweets together — yours and others’ — to create a short story. It’s a bit like Storify, which recently lost its battle with cancer … er … capitalism. RIP, brave fighter! ; )
Discovered a new Twitter tool that I’m geeking out about a little. It’s called ‘Moments’ and it lets you string a bunch of tweets together — yours and others’ — to create a short story. It’s a bit like Storify, which recently lost its battle with cancer … er … capitalism. RIP, brave fighter! ; )
 Here’s my
Here’s my